
Last chance for a critical patient
Barcelona, October 4, 2023
Dr FERNANDO JUAN GERBER
On September 2023, we carried out a secondary transfer of a 45-year-old patient from Senegal to Spain.
Status report
The patient was a patient with a history of pleural tuberculosis in 2016 and COVID-19 lung disease in June 2023.
Currently, the patient was admitted to the intensive care unit in Senegal with a requirement for invasive mechanical ventilation since September 9 with a diagnosis of diffuse lung disease without associated organ failure.
Preparation for the transfer
The collection of information was quite difficult, the language barrier, the disparity of pathophysiological concepts for the diagnosis and treatment of the pathology to be treated and the availability of resources at the destination, made it difficult to diagnose the patient’s real situation.

With the information collected, we defined that the patient was a 45-year-old patient with a history of acute lung disease and who was currently experiencing adult respiratory distress syndrome with persistent hypoxemia and hypercapnea, associated with pneumothorax of the right lung field without associated organ failures.
The day before departure, at the Aeromedical and Marine TRI facilities, we held a mission briefing based on the information collected at the time. Transfer decision, modality, requirements, etc. a check of electromedicine and supplies, including verification via checklist of medication and consumables as well as testing of electronic equipment, batteries and connections to an electrical source.
Already at the airport we transfer electromedicine and supplies to the aircraft, we check respirator connections and electrical connectivity to the aircraft stretcher.
Crew briefing
Pilots present flight plan, schedules, flight profile, safety measures.
Aeromedical personnel raised the secondary transfer situation, aircraft requirements for the transfer, updating information on the patient’s global situation and the family and hospital environment.
We arrived at the airport in Senegal without incident. The transfer picked us up on time and took us to the hospital where the patient was for an assessment prior to the transfer.
Once there we prepared to enter the intensive care unit, we corroborated the information previously received but the severity of the situation was underestimated by the unit’s treating staff.
This was a 45-year-old patient with a history of acute lung disease who was currently experiencing adult respiratory distress syndrome with refractory hypoxemia and a large bronchopleural fistula.

Transfer
On October 23, early in the morning, we met on the tarmac with the ambulance that brought us the patient from the ICU. The patient was in the same condition as the night before. The ambulance doctor told us that the patient spent the entire night awake, struggling with mechanical ventilation and having an oxygenation crisis.
Before boarding the aircraft, we explained to the patient that we would put him to sleep and that we were going to travel by plane to another country to help resolve his condition.
We did a quick briefing of the crew, pilots and aeromedical personnel, we explained to the ambulance and runway personnel the steps to follow for the transfer. We established an action plan.
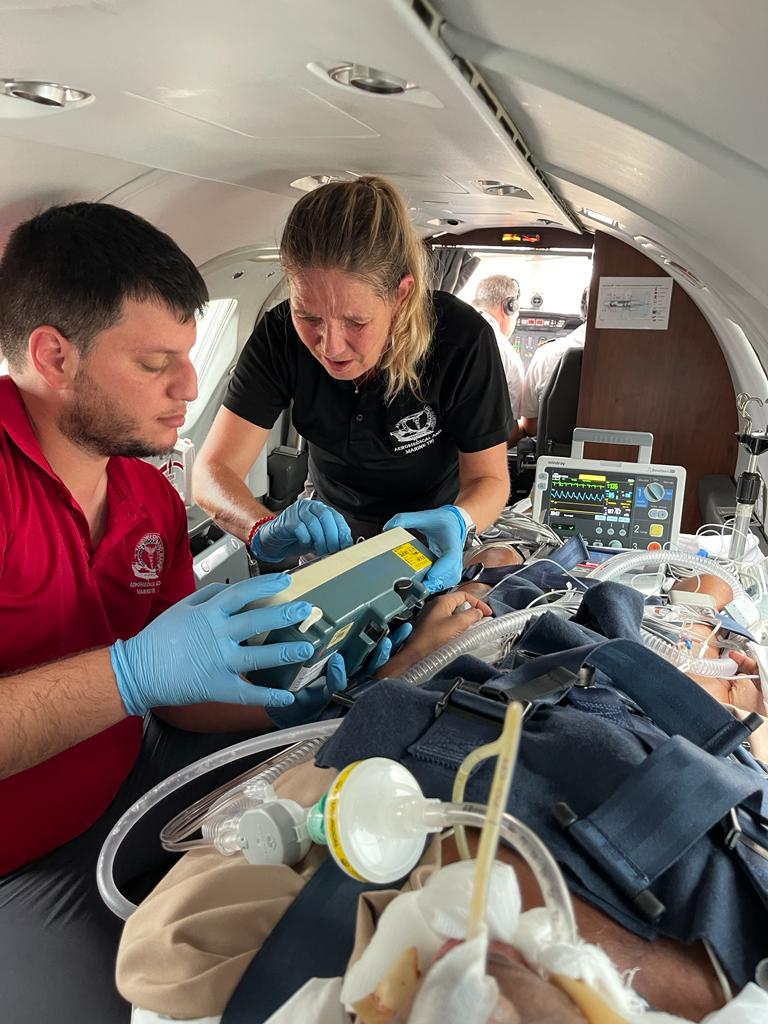
We performed deep sedation and neuromuscular blockade on the patient, then we transferred electromedicine. We optimized mechanical ventilation and quickly obtained respiratory improvement.
Once on the plane we conditioned all the devices, vascular access, respiratory orotracheal tube and pleural drainage, we replaced fixations, we sanitized the oral cavity that had large pressure ulcers from the oral device. Bladder and nasogastric tube.
During the transfer we reinforced prophylactic anticoagulation and stimulate a diuretic rhythm. We reinforced corticotherapy.
 Finally, after 7 hours 50 minutes, requiring a stopover in the Canary Islands to supply fuel and oxygen, we arrived in Madrid. We transferred her to an ambulance that took her to the ICU at her destination without incident.
Finally, after 7 hours 50 minutes, requiring a stopover in the Canary Islands to supply fuel and oxygen, we arrived in Madrid. We transferred her to an ambulance that took her to the ICU at her destination without incident.
Final diagnosis
1) ARDS with refractory hypoxemia
2) Bronchopleural fistula
Dr FERNANDO JUAN GERBER
