

Medical Escort Support for VIP Tourism; A Dream Cruise Along The Nile
At Aeromedical and Marine TRI, we specialize in medical repatriations, ensuring the safe and efficient return of patients to their home countries. However, we occasionally have the opportunity to provide unique and extraordinary services beyond our usual scope. Recently, we had the privilege of offering VIP medical escort support to our patient, Steve, as he embarked on a dream cruise along the Nile in Egypt. This experience highlights a special aspect of our services, where we combine medical expertise with personalized care to fulfil our patient’s extraordinary travel aspirations.
Each mission we undertake is unique, but this time we had a very special mission: fulfilling a dream. Our patient contacted us because he had an unfulfilled dream of travelling to Egypt to photograph its mysterious pyramids and temples. However, his health condition prevented him from making the trip on his own, so he asked us if we could help him make it come true.

I was assigned the mission as a nurse escort, and together with the rest of the team, we began working on finding a way to make the trip safely. First, we reviewed the patient’s medical history. He was a multi-pathological patient, actively undergoing cancer treatment for leukaemia, with an old below-knee amputation of his left leg and a prosthesis, which allowed him relatively autonomous mobility thanks to strict rehabilitation. However, two weeks before the trip, he had to undergo an amputation of two toes on his right foot due to diabetic foot, significantly limiting his mobility and increasing the risks during the trip, primarily infection and sepsis. Therefore, we planned to provide daily wound care and assessments.


The trip was organized by an agency and consisted of 12 days of travel, with numerous transfers (8 flights, 7 days of cruising, and almost daily coach trips for excursions). Egypt, moreover, does not have infrastructures adapted for people with reduced mobility nor a quality healthcare system in most of the territory, often presents inadequate sanitary conditions, and extreme temperatures of up to 43ºC. Thus, our challenge was to find solutions to these difficulties without leaving room for unforeseen events, for which we had alternative plans in case of need, including repatriating the patient to Barcelona for hospital medical care, mobilizing the necessary resources depending on the point of the route we were on: in the middle of the Nile cruise, in the city, or in more remote desert areas. All chances were considered to act with the greatest speed and safety possible.


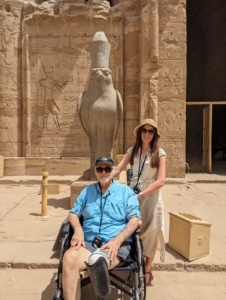
Finally, the greatest challenge during the trip was mobility. Transfers and excursions, in some cases, were more demanding than anticipated due to the instability of the terrain, combined with the heat and the patient’s weakness in the first days after the oncological treatment administered just before the trip. For this reason, we adapted the pace of the trip each day, thus being able to enjoy every moment. On some days, when we had more energy, we enjoyed incredible excursions and visits, and on other days, we simply enjoyed a good conversation and photographed an unforgettable sunset on the Nile from the cabin balcony, recovering strength for the next adventure.

We can proudly say that the mission was accomplished beyond expectations. We fulfilled a dream, overcame all the obstacles that arose, always keeping the situation under control, and enjoyed a wonderful and enriching experience for all. The greatest reward is seeing the happiness of our patient, and now, friend.

From Aeromedical and Marine we love you, Steve, and above all we admire your strength, determination and courage to fulfil your dreams and purposes. See you very soon!
Arantxa Moreno Panella_Nurse in charge of the mission


“Calgary – Karachi, Navigating Language and Cultural Challenges: A Report of Successful Aeromedical Repatriation”
In the world of aeromedical repatriation, every mission carries its own unique set of challenges. However, some journeys stand out for their exceptional complexity and the resilience required to overcome them. Such was the case with a recent mission undertaken by Aeromedical and Marine TRI INT, involving the repatriation of our patient, from Calgary, Canada to Karachi, Pakistan, via Abu Dhabi.
Our patient, a 68-year-old man originally from Pakistan, had been battling sepsis. Though the medical issue had been resolved, he remained in fragile condition, necessitating careful transport back to his homeland. What made this mission particularly a challenge was not just the medical condition of the patient, but the language and cultural that loomed large.
With our patient speaking primarily Gujarati, communication presented a significant challenge. However, the team at Aeromedical and Marine TRI INT approached the task with determination and resourcefulness. Despite the linguistic hurdles, effective communication channels were established, ensuring that the patient needs were understood and addressed throughout the journey.

The team’s cultural sensitivity and adaptability proved invaluable in fostering trust and cooperation with our patient and his family. This ensured a smoother process and eased any anxieties associated with the repatriation.
Despite meticulous planning, the journey encountered an unexpected obstacle when the flight was delayed by nearly 24 hours. However, the team remained steadfast, ensuring that our patient received the necessary care and attention during the extended wait.
In the end, the mission was a testament to the professionalism and dedication of the Aeromedical and Marine TRI INT team. Despite the challenges, they navigated through with grace and determination, ensuring the safe repatriation of our patient to his homeland.

Aerial Night View of Karachi. César Garcia
As we reflect on this mission, it serves as a reminder of the importance of empathy, adaptability, and collaboration in overcoming even the most daunting of obstacles. Through effective communication and cultural understanding, we can bridge divides and ensure the well-being of those in need, no matter the distance or barriers faced.

GREAT HONOUR FOR THE AEROMEDICAL & MARINE TRI SL / USA LLC 2024 GLOBAL RECOGNITION AWARD
From Aeromedical and Marine TRI, we feel deeply grateful for the recognition received in the Global Recognition Award™ 2024
We would like to express our deep thank you to the esteemed members of the Global Recognition Award™ 2024 jury.
On behalf of Aeromedical And Marine TRI, I extend our heartfelt gratitude to each one of you for honouring us with the esteemed Global Recognition Award™ for 2024. It is with immense pride and gratitude that we receive this recognition for our unwavering commitment to excellence in service provision and outstanding results.
We are deeply humbled by this prestigious accolade, which serves as a testament to the dedication and hard work of every member of our team. At Aeromedical And Marine TRI, we strive relentlessly to uphold the highest standards of quality and innovation in our services, and this award reaffirms that our efforts have not gone unnoticed.
Your recognition not only validates our ongoing endeavours but also inspires us to continue pushing the boundaries of excellence in the field of aeromedical and marine repatriations services. It is truly an honour to be acknowledged by such a distinguished panel of industry experts, and we are immensely grateful for the opportunity to showcase our achievements on a global platform.
Once again, thank you for bestowing this remarkable honour upon Aeromedical And Marine TRI. We are deeply appreciative of your support and encouragement, and we remain committed to delivering unparalleled excellence in all aspects of our work.
With sincere gratitude,
Aeromedical & Marine TRI SL
Aeromedical & Marine TRI USA LLC

Here you can read the full text of the jury members about our award-winning work:
Aeromedical & Marine TRI SL / USA LLC has been recognized with a 2024 Global Recognition Award for its exceptional contributions to the medical assistance provider industry, especially in the fields of air and maritime medical evacuations, repatriations, and personalized medical escort support. Operating from Spain, the company has shown remarkable growth and quality of service, significantly impacting the global scene. With an annual revenue contact of 1.8M and an impressive revenue increase of 1000%, Aeromedical & Marine TRI SL / USA LLC has broadened its reach and established a new benchmark in delivering crucial medical services to those in need.
Boasting over 150 clients since its foundation, Aeromedical & Marine TRI SL / USA LLC is distinguished for its dedication to excellence and its capability to provide round-the-clock service for aeromedical, marine, or VIP medical evacuation/escort requests. The firm’s customized medical network, concentrating on various medical and surgical specialties, including trauma recovery, ensures each client receives the most advanced and personalized care. This commitment to patient care and service innovation positions Aeromedical & Marine TRI SL / USA LLC as a leader in its domain and a deserved recipient of the 2024 Global Recognition Award.
Innovation and Leadership in the Industry
Aeromedical & Marine TRI SL / USA LLC’s forward-thinking approach to medical assistance highlights its leadership within the industry. The company has tackled the challenges of providing top-tier, efficient medical evacuation and escort services across air and maritime environments. Their focus on ensuring accessibility to their services, combined with an emphasis on quality and efficiency, illustrates an inventive strategy for overcoming logistical and operational hurdles in the medical evacuation field. This inventive mindset improves client safety and well-being and propels the industry forward, inspiring others to adopt similar practices.
Their specialized offering of dedicated medical air escorts for VIP clients seeking personal medical support demonstrates Aeromedical & Marine TRI SL / USA LLC’s role in catering to niche markets within the medical assistance industry. By providing customized services that cater to the unique needs of VIP clients, Aeromedical & Marine TRI SL / USA LLC not only broadens its market presence but also solidifies its reputation as a versatile and client-centered provider. This strategic diversification of services is one of the main reasons for their selection as 2024 Global Recognition Award recipients, highlighting their pioneering efforts in the medical assistance provider industry.
Client and Community Impact
Aeromedical & Marine TRI SL / USA LLC’s significant impact on its clients and the larger community is profound. Through their comprehensive services, they have saved lives and offered crucial support in critical moments. The company’s readiness and efficiency in responding to emergencies, regardless of location or complexity, reflect its deep commitment to its mission. This steadfast dedication to positively influencing the lives of individuals and families during their most vulnerable times is foundational to their corporate ethos and a crucial reason for their award recognition.
Furthermore, Aeromedical & Marine TRI SL / USA LLC’s work extends beyond the immediate benefits of their services. By setting high standards in the medical evacuation and escort industry, they contribute to a broader ecosystem of safety, reliability, and care within the medical community. Their efforts benefit their direct clients and promote advancements in medical care and emergency response strategies, benefiting the industry at large. The widespread effect of their dedication and quality of service emphasizes the significant and broad impact Aeromedical & Marine TRI SL / USA LLC has had, making them a fitting recipient of the 2024 Global Recognition Award.
Final Words
Receiving the 2024 Global Recognition Award reflects Aeromedical & Marine TRI SL / USA LLC’s excellence in innovation, leadership, and influence within the medical assistance provider industry. Their remarkable growth, client-focused services, and adherence to quality and efficiency distinguish them as a leading example of excellence. As they continue to expand their services and influence, Aeromedical & Marine TRI SL / USA LLC remains a prime example of how dedication, innovation, and a focus on client care can lead to significant success and make a meaningful difference in the world.
Their forward-looking approach and steady focus on enhancing the health and safety of their clients have rightfully earned them this accolade. As Aeromedical & Marine TRI SL / USA LLC progresses, its path reflects not just past achievements but also a guide for future initiatives in the global medical assistance field. The 2024 Global Recognition Award is a well-earned recognition of their substantial contributions and indicates the more groundbreaking and impactful work yet to come.
LINK TO THE Global Recognition Award™ 2024
![]()




At Aero Medical & Marine Training and Rescue International, we handle diverse and complex missions across the globe, each one with its unique challenges and moments of deep human connection.
One recent mission took us to Kilimanjaro, Tanzania, where a patient sustained serious injuries after a fall during a safari expedition. Thanks to the incredible expertise and dedication of Alexia Hartmann Fernández, who traveled from Spain to personally lead the repatriation, the patient and her family were safely transported to Denmark.
From remote terrain and cross-border coordination to detailed medical planning, this mission was a testament to the resilience of our team and the strength of collaboration. Every procedure, every detail, every mile handled with care, precision, and compassion.
This is just one of many stories that remind us why we do what we do.







